202406202130
Status:
Tags: pharmacology
Opioid
Opioids induced hyperalgesia vs tolerance
Frequently confused but often co-exist
Both manifest clinically as need for ↑opioid dose to achieve same analgesic effect
- tolerance → give ↑ dose
- OIH → avoid opioids, & use other analgesics or adjuncts
- ↑ opioid → ↑ pain
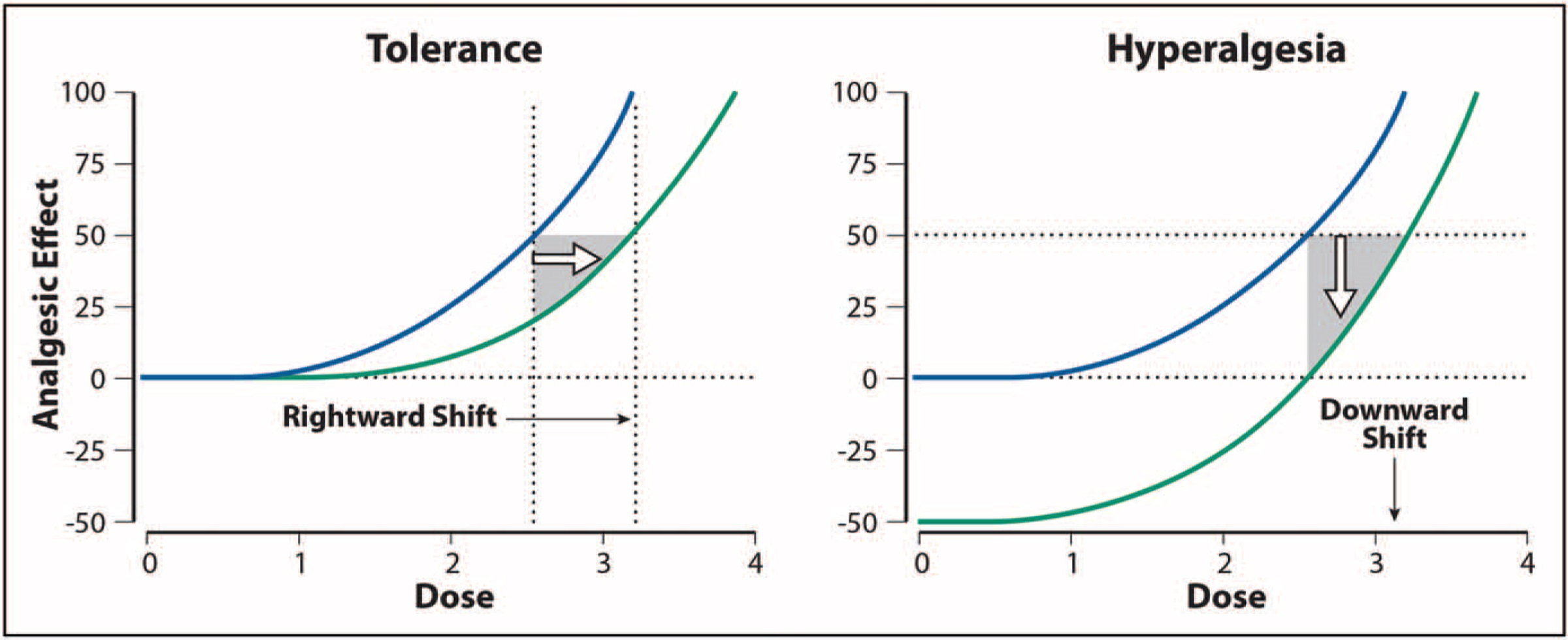
Dose-effect relationship: Tolerance shifts to right (but dose not alter pain sensitivity). OIH shifts down ∵ ↑pain sensitivity
- ↑ opioid → ↑ pain
OIH
also read: Remifentanil#Remifentanil induced hyperalgesia
Definition: a state of paradoxically ↑ response to noxious stimuli, presumably as a result of nociceptive sensitisation, caused by an exposure to opioids
a "normal adaptive response" counteracting perturbations from exogenous opioids?
a/w nearly all types of opioids, w/ dose-dependent hypersensitivity e.g.
- morphine-6 glucuronide
- methadone
- phenanthrene-based class opioids
- synthetic opioids-piperidines
- NOT w/ oxymorphone
OIH incidence & degree of hyperalgesia ∝ opioid dose & exposure duration
Possible mechanisms
predominance of pronociceptive mechanisms e.g. activation of NMDA system
on > off-neurons w/i rostro-ventral medulla
- descending spinal facilitation
- mediated via NMDA system
- exposure to prolonged noxious stimuli induced "on" state
- µ opioid receptor ligand → "off" state
↑ dynorphin in spinal cord & primary afferents after noxious stimuli activate release of calcitonin gene related peptide
Remifentanil: activates peripheral & spinal neurons differently, which presumably results in hyperalgesia developing at different time point (early vs late) during post-infusion period.
Table 1 - Cellular mechanisms potentially responsible for the development of OIH
| μ-Opioid signaling | ↑cAMP & protein, kinase A Protein kinase C, C-Jun N-terminal kinase β-Arrestin-2 SRC kinase |
|---|---|
| Transcriptional mechanisms | cAMP response element-binding protein Mammalian target of rapamycin complex 1 |
| Pronociceptive ion channels | NMDA receptors Transient receptor potential vanilloid channels |
| Microglia | Toll-like receptor 4 P2X4 and P2X7 purinergic receptors Brain-derived neurotrophic factor Scaffold protein β-arrestin-2 |
Prevention & treatment
General
↓ opioid dose & gradual dose tapering
NMDA antagonists
- ketamine
- 5 µg/kg/min infusion effective for Remifentanil
- dextromethorphan
Buprenorphine - κ-receptor agonism
- δ-receptor downregulation
- 25 µg/h for 24h for RIH
COX-2 inhibitor - Parecoxib
- effective w/ early treatment 30min before application of remi
- concomitant administration ineffective?
α2 agonists - Dexmedetomidine
methadone
MgSO4
RIH
Gradual taper of Remifentanil infusion rate (vs abrupt stop)
addition of Propofol to Remifentanil may ↓OIH
- ? ∵ inhibitory effects on NMDA receptors
- effect on supraspinal GABA-A receptors
- even sub-hypnotic dose may help
Opioid tolerance
References
Remifentanil-Induced Hyperalgesia The Current State of Affairs